OIG Report Offers Glimpse into CMS Progress Towards MACRA Implementation
Last week, the Office of Inspector General (OIG) of the U.S. Department of Health and Human Services released a report analyzing CMS' readiness to implement major parts of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA). The report provides an inside look at the steps CMS is taking to implement MACRA's Quality Payment Program (QPP), which is an ambitious transformation of the way in which the federal government reimbursements health care providers. The report highlights two key vulnerabilities for the MACRA transition, a process that will hopefully be smoother than the troubled roll out of HealthCare.gov.
MACRA Refresher
Starting in 2019, the QPP will replace a number of existing reporting programs with a two-track system under which eligible clinicians will receive incentive reimbursement payments through either:
- The Merit-Based Incentive Payment Systems (MIPS); or
- Advanced alternative payment models (APMs).
Under MIPS, eligible clinicians can receive incentive payment (or penalty) based on four categories of measures: quality, cost, improvement activities, and the use of EHRs. Alternatively, clinicians can be reimbursed under the second track if they participate in an “Advanced APM.” Advanced APMs include certain accountable care organizations (ACOs) and patient-centered medical homes. For a full discussion of the QPP, MIPS and APMs, see our post on CMS' final rule.
OIG's Findings
From interviews with CMS leadership and staff and analysis of key documents, OIG identified CMS’ five key management priorities regarding the planning and early implementation of the QPP. These priorities include:
- fostering clinician acceptance and readiness to participate;
- adopting integrated internal business practices to accommodate a flexible, user-centric approach;
- developing IT systems that support and streamline clinician participation;
- developing flexible and transparent MIPS policies; and
- facilitating participation in Advanced APMs.
1. Fostering Clinician Acceptance
The OIG found that CMS has taken a number of steps to foster clinician acceptance and readiness, including engaging clinicians and stakeholders, conducting user testing of the QPP Portal (discussed below), establishing "Clinician Champions," creating a transition year, and awarding contracts for education, support and technical assistance. As we noted in our prior post, the creation of the transition year will give clinicians the ability to submit only a minimum amount of data for 2017 without the threat of a negative payment adjustment.
Of the two vulnerabilities identified in the report, one is found within this management priority. The vulnerability relates to CMS ability to conduct outreach and provide technical assistance so that providers--especially solo, small-practice, and rural providers--have the information they need. In the OIG's words:
If providers lack the knowledge, tools, or skills to participate, they will struggle to meet the QPP reporting requirements. Frustrated providers may even opt not to participate in the QPP despite the payment penalty, limiting the program’s ability to meet its goals. To mitigate this risk, CMS must continue to monitor clinician readiness—especially as the first reporting deadline approaches—to identify and address any problems early on. CMS has begun its technical assistance and training efforts, but these activities must quickly be ramped up to full scale and continued throughout 2017 to support Medicare clinicians’ participation in the QPP.
2. Adopting Integrated, Flexible Business Practices
As the OIG notes, implementing the QPP requires CMS to coordinate policy, technology, communications, and operations activities. Additionally, because the legacy programs on which the QPP is based are dispersed among various CMS components, staff with necessary expertise and experience are similarly dispersed. Staff working with many of the APMs, for example, report to the CMS Center for Medicare & Medicaid Innovation, while those involved in the Value-Based Payment Modifier program are located in the CMS Center for Medicare. To address this logistical and organizational complexity, the report describes how CMS sought to learn from the problems of HealthCare.gov by adopting an integrated, flexible approach to both program management and IT development. To create this flexible management approach, CMS developed an overall QPP strategy, assigned executive leadership to each program component, established integrated project teams with shared office space, adopted agile IT development methods, adopted a new contracting approach, and awarded a systems integrator contract. According to the report, CMS is still planning on awarding additional contracts, expanding oversight of contractors, and hiring staff with expertise in agile development.
3. Developing IT Systems
Information technology is arguably CMS' greatest hurdle to a successful QPP roll out. Front and center to CMS' IT efforts is the QPP Portal. This portal will consist of three major components: a public-facing informational website, individualized accounts for clinicians, and backend systems necessary to receive and validate clinicians' data, provide individualized performance feedback, calculate clinicians' MIPS scores, and adjust Part B payments accordingly. 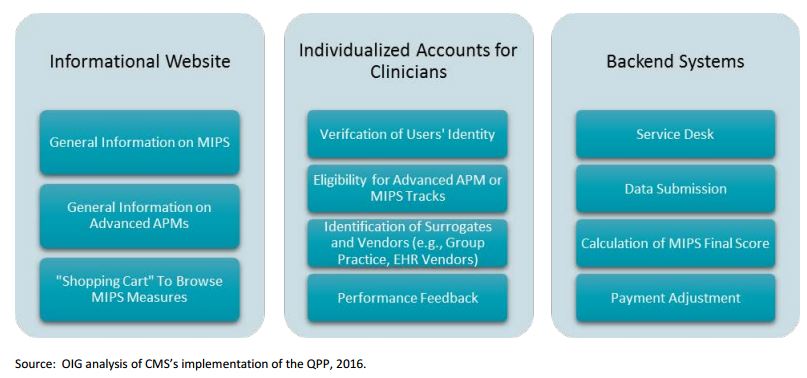
CMS launched the informational website in October 2016. However CMS has yet to enable the individualized accounts or set up the backend systems. CMS staff have reported to OIG that individualized accounts will indeed be available in January 2017. These accounts will ultimately enable CMS to verify the user’s identity, inform clinicians of their eligibility for the Advanced APM track versus the MIPS track (so that clinicians know whether they must select and report MIPS measures), and provide individualized performance feedback.
OIG identified the development of the backend IT system as the second of the two vulnerabilities to the QPP's roll out, noting in its report that:
Building and testing the extensive IT systems necessary to support critical QPP operations will require significant and sustained effort over the forthcoming year. In the past, CMS has sometimes experienced delays and complications related to major IT initiatives, such as those required for the continued operation of Medicare Part D and HealthCare.gov. If the complex systems underlying the QPP are not operational on schedule, the program will struggle to meet its goal of improving value and quality.
According to the report, CMS plans to partially mitigate this risk by using the legacy systems for the existing reporting programs as a backup option for MIPS data submission.
4. Develop MIPS Policies
OIG noted that CMS was able to issue a final rule, including policies on MIPS, notwithstanding a challenging deadline and a massive number of public comments. OIG identified three future initiatives under this management priority, including issuing promised subregulatory guidance, finalizing policies for so-called "virtual groups," and subsequent rulemaking in 2018 and beyond.
5. Facilitate Participation in Advanced APMs
OIG's report identifies a number of steps that CMS has taken to address this management priority, including:
- identifying which existing Medicare models meet criteria for Advanced APMs;
- establishing policy for determining Qualifying APM Participants;
- publishing the Final Rule, including Advanced APM policies for 2017; and
- awarding contracts for technical assistance to prepare clinicians to participate in Advanced APMs.
The report lists a number of initiatives that remain, including determining which clinicians are Qualifying APM Participants, increasing Advanced APM opportunities, and increasing clinician participation in Advanced APMs over time.
Commentary
This report is both reassuring and concerning. On the one hand, OIG concludes that CMS has made significant progress towards implementing the QPP, and has done so by addressing many of the key lessons learned from the troubled launch of HealthCare.gov. These steps will undoubtedly allow CMS to respond more quickly to problems as they arise. On the other hand, OIG still believes that vulnerabilities exist with respect to both clinician engagement and the QPP's backend IT systems. A successful QPP roll out could also be affected by the new administration. Budget cuts and/or organizational changes at CMS may affect the agency's ability to respond to the identified vulnerabilities. A new administration could also place restrictions on the agency's power to create new Advanced APMs, which could create a new vulnerability at the heart of the QPP's policy objective.